What Is Ventricular Fibrillation?
Your heart depends on a precise electrical system to keep it beating in a steady rhythm. With every heartbeat, an electrical signal travels through the heart muscle in an orderly pattern, telling the chambers when to contract and push blood to the lungs, brain, and the rest of your body. Ventricular fibrillation, often called v fib, is what happens when that electrical system fails completely.
During ventricular fibrillation, the lower chambers of the heart (the ventricles) receive rapid, chaotic electrical signals. Instead of contracting in a coordinated way, the ventricles quiver and twitch uselessly. No blood gets pumped. Within seconds, the person loses consciousness. Within minutes, without treatment, the brain and organs begin to suffer irreversible damage. This is sudden cardiac arrest, and v fib is the most common rhythm behind it.
Here is the critical point: ventricular fibrillation is not a heart attack. A heart attack happens when a blocked artery cuts off blood supply to part of the heart muscle. A heart attack can trigger v fib, but v fib is an electrical problem, not a plumbing problem. This distinction matters because the treatments are different. A heart attack needs a hospital. V fib needs an immediate shock from a defibrillator, and every second counts.
If you or your organization is responsible for the safety of others, having an AED (automated external defibrillator) on-site is one of the most important steps you can take. Learn how to use an AED in an emergency.
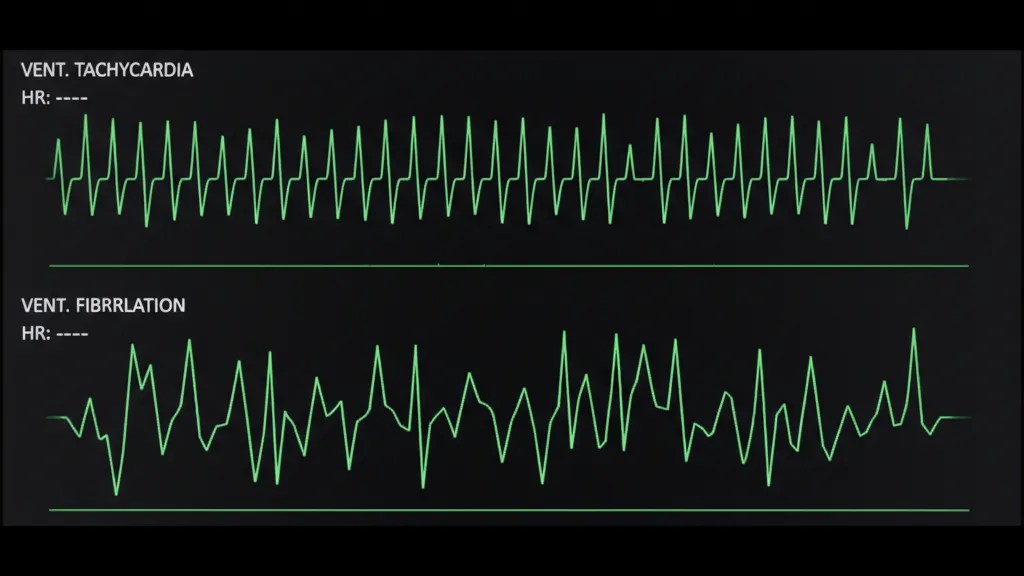
Ventricular Fibrillation vs. Ventricular Tachycardia: What Is the Difference?
Two dangerous heart rhythms are commonly discussed together: ventricular fibrillation (v fib) and ventricular tachycardia (v tach). Both originate in the ventricles and both can be life-threatening, but they are different conditions.
Ventricular tachycardia (v tach) is a rapid but still organized heartbeat originating in the ventricles. The heart may beat 150 to 250 times per minute. In some cases, the person remains conscious and has a pulse, though they may feel dizzy, short of breath, or experience chest pain. Sustained v tach is dangerous because the heart is beating so fast it cannot fill with enough blood between beats, reducing blood flow to the body.
Ventricular fibrillation (v fib) is completely disorganized. There is no recognizable heartbeat pattern at all. The ventricles simply quiver, producing no effective blood flow. A person in v fib has no pulse, is unconscious, and is in cardiac arrest. Without immediate defibrillation, v fib is fatal.
The key relationship between these two rhythms is that v tach often deteriorates into v fib. What may start as a dangerously fast but organized rhythm can collapse into total electrical chaos. This is why both rhythms are considered “shockable” by an AED. An automated external defibrillator is designed to analyze the heart’s electrical activity and determine whether a shock can help. If it detects either v fib or pulseless v tach, it will advise delivering a shock.
Symptoms and Warning Signs
Ventricular fibrillation itself happens suddenly and without warning in most cases. The person collapses, becomes unresponsive, and stops breathing normally. There is no pulse. This is a medical emergency that requires an immediate 911 call, CPR, and defibrillation.
However, some people experience warning signs in the minutes or hours before v fib occurs:
- Chest pain or pressure
- Rapid or pounding heartbeat (palpitations)
- Dizziness or lightheadedness
- Shortness of breath
- Nausea
- Fainting or near-fainting
These symptoms may indicate an underlying heart problem, such as a heart attack in progress, that could trigger v fib. Anyone experiencing these symptoms should seek medical attention immediately. If someone near you suddenly collapses and is unresponsive, assume the worst and act fast. Call 911, start CPR, and use an AED if one is available.
What Causes Ventricular Fibrillation?
V fib rarely happens in a perfectly healthy heart. It is almost always triggered by an underlying condition that disrupts the heart’s electrical system. The most common causes include:
Coronary artery disease: This is the leading cause of v fib. When the arteries supplying blood to the heart become narrowed or blocked by plaque, the heart muscle can become damaged or oxygen-starved. This damage creates areas where electrical signals can go haywire, triggering v fib.
Heart attack (myocardial infarction): A heart attack can directly trigger ventricular fibrillation. During a heart attack, the dying heart tissue disrupts normal electrical pathways, and v fib can occur during or shortly after the event. This is why many cardiac arrest deaths happen within the first hour of a heart attack.
Cardiomyopathy: This term describes diseases of the heart muscle itself. Whether the heart is enlarged, thickened, or stiffened, the structural changes can create conditions where abnormal electrical circuits form, increasing the risk of v fib.
Heart valve disease: Damaged or malfunctioning heart valves force the heart to work harder, which can weaken the muscle over time and increase the risk of dangerous rhythms.
Congenital heart conditions: Some people are born with electrical abnormalities in their hearts, such as Long QT Syndrome or Brugada Syndrome, that make them susceptible to v fib, sometimes at a young age.
Electrolyte imbalances: Your heart’s electrical system depends on a balance of minerals like potassium, magnesium, and calcium. Severe imbalances from dehydration, kidney disease, or certain medications can destabilize the rhythm.
Drug and substance use: Certain drugs, including some prescription medications, recreational stimulants, and excessive alcohol, can trigger or increase the risk of ventricular fibrillation.
Risk Factors for V Fib
While v fib can technically happen to anyone, certain groups face a higher risk:
- Previous heart attack: Scar tissue from a prior heart attack creates areas of abnormal electrical activity in the heart
- History of heart disease: Coronary artery disease, heart failure, or cardiomyopathy all increase risk
- Family history of sudden cardiac arrest: A genetic component exists, especially with inherited conditions like Long QT Syndrome
- Age: Risk increases with age, though sudden cardiac arrest can occur in young athletes and children
- Electrolyte disorders: Chronic kidney disease or conditions causing potassium or magnesium imbalances
- Drug use: Stimulants like cocaine and methamphetamine significantly raise the risk
- Previous episode of v fib or v tach: Having survived one episode increases the chance of another
Understanding these risk factors matters for individuals and organizations. If your workplace has employees over 40, or if your community center serves an aging population, cardiac emergencies will happen. Being prepared with an AED and trained staff is not optional.
Preparedness saves lives. Equip your workplace, school, or community space with an AED package that includes everything you need: the defibrillator, a wall cabinet, signage, and a first responder kit. Contact Response Ready to find the right solution.
How AEDs Detect and Treat Ventricular Fibrillation
An automated external defibrillator is engineered to treat ventricular fibrillation. Understanding how it works helps you appreciate why these devices are effective and safe for anyone to use.
Step 1: Heart rhythm analysis. When you place the AED pads on a person’s bare chest, the device immediately begins reading the heart’s electrical activity through the skin. The AED’s computer analyzes this electrical signal using sophisticated algorithms that can distinguish between a normal rhythm, a shockable rhythm (v fib or pulseless v tach), and a non-shockable rhythm (like asystole, which is a flatline).
Step 2: Shock decision. If the AED detects ventricular fibrillation, it charges its capacitor and either delivers a shock automatically or prompts the user to press the shock button, depending on the model. If the rhythm is not shockable, the AED will not allow a shock to be delivered. This built-in safety feature means you cannot accidentally harm someone with an AED.
Step 3: Defibrillation. The shock itself is a controlled burst of electrical energy delivered through the chest and into the heart. The goal is not to “restart” the heart like a jump-start. Instead, the shock momentarily stops all electrical activity in the heart, giving the heart’s natural pacemaker cells a chance to re-establish an organized rhythm. Think of it as pressing a reset button on a frozen computer.
Step 4: CPR and reassessment. After the shock, the AED will instruct the rescuer to perform CPR for two minutes, then it will re-analyze the rhythm. This cycle of shock, CPR, and analysis continues until emergency medical services arrive or the heart returns to a normal rhythm.
Modern AEDs from leading manufacturers like Philips, ZOLL, HeartSine, Stryker, Cardiac Science, and Defibtech are designed with clear voice prompts, visual indicators, and intuitive pad placement diagrams that guide even untrained bystanders through every step. Some models also include real-time CPR feedback technology that coaches you on compression depth and rate, further improving outcomes.
Survival Rates: Why Every Second Matters
The statistics around sudden cardiac arrest and ventricular fibrillation are sobering, but they reveal a clear path to saving more lives.
According to the American Heart Association, more than 350,000 out-of-hospital cardiac arrests occur in the United States each year. The overall survival rate is about 10%. When a bystander uses an AED before EMS arrives, survival jumps to between 50% and 74%.
The difference comes down to time. For every minute that passes without defibrillation, the chance of survival decreases by 7% to 10%. After 10 minutes without a shock, survival is unlikely. The average EMS response time in the United States is 7 to 14 minutes, depending on location. In rural areas, it can be even longer.
This is why public access defibrillation programs exist. When AEDs are placed in schools, offices, gyms, airports, churches, and community centers, the time to first shock drops dramatically. A bystander can retrieve an AED and deliver a shock in 3 to 5 minutes, well within the window where survival rates are highest.
The data tells a simple story: the best chance of surviving v fib is an AED that is close by, accessible, and ready. Read more about how AED accessibility impacts survival.
Response Ready carries AEDs from all six FDA-approved manufacturers, so you can find the right device for your environment and budget. Browse AED devices or call us at 858-665-2025 for personalized guidance.

What to Do If You Witness a Cardiac Arrest
If someone near you suddenly collapses, is unresponsive, and is not breathing normally, follow these steps:
- Call 911 immediately (or ask someone nearby to call)
- Start CPR: Push hard and fast in the center of the chest, at least 2 inches deep, at a rate of 100 to 120 compressions per minute
- Send someone for an AED: If one is nearby, have someone retrieve it while you continue CPR
- Use the AED: Turn it on, follow the voice prompts, attach the pads to the bare chest, and let the device analyze the rhythm. If it advises a shock, make sure no one is touching the person, and press the shock button
- Continue CPR: Resume compressions immediately after the shock and continue until EMS arrives or the person begins to move and breathe normally
You do not need medical training to use an AED. The device guides you through every step. You cannot make a mistake that harms the patient, because the AED will only shock a rhythm that requires it. The biggest mistake you can make is doing nothing.
For those who want to build confidence, CPR and AED training courses are available through Response Ready’s nationwide network of certified instructors. Training gives you hands-on practice so you can act without hesitation when it counts.
Frequently Asked Questions
Can ventricular fibrillation happen to young, healthy people?
Yes. While v fib is more common in people with existing heart conditions, it can affect young people, including athletes. Inherited conditions like Long QT Syndrome, Hypertrophic Cardiomyopathy, or a sudden blow to the chest (commotio cordis) can trigger v fib in otherwise healthy individuals. This is why AEDs in schools, sports facilities, and youth athletic events are so important.
Is ventricular fibrillation the same as a heart attack?
No. A heart attack is caused by a blocked artery cutting off blood flow to the heart muscle. Ventricular fibrillation is a chaotic electrical malfunction that stops the heart from pumping blood. A heart attack can cause v fib, but they are different conditions. V fib requires defibrillation; a heart attack requires emergency medical care at a hospital.
Can you survive ventricular fibrillation without an AED?
Survival without defibrillation is extremely unlikely. CPR alone can buy time by manually circulating some blood, but CPR cannot correct the chaotic electrical activity of v fib. Only a defibrillator can reset the heart’s rhythm. The combination of early CPR plus early defibrillation gives the best chance of survival.
How much does an AED cost?
AEDs from FDA-approved manufacturers typically range from $1,400 to $2,900, depending on the model and features. Response Ready also offers complete buying guides and value packages that bundle the AED with a cabinet, signage, and accessories to simplify the process.
Do AEDs require maintenance?
Yes, but maintenance is minimal. AED pads and batteries have expiration dates and need periodic replacement. Most modern AEDs perform daily self-checks and display a status indicator showing whether the device is ready. Response Ready’s AED Total Solution program provides ongoing compliance management, so you never have to worry about tracking expiration dates yourself.